The Joint Annual Scientific Meetings of the Endocrine Society of Australia and the Society for Reproductive Biology 2018
Disproportionate Hypertriglyceridaemia in a patient with Familial Lipodystrophy (#234)
A 35 year old lady with a heart transplant in 2015 for dilated cardiomyopathy cardiomyopathy secondary to familial partial lipodystrophy (Dunnigan type- confirmed LMNA gene mutation) was admitted to hospital with features of congestive cardiac failure.
Complications include post transplant diabetes, fatty liver disease, hypertension, paroxysmal atrial flutter and steroid-related osteopenia. Medications include prednisone 9mg/day, tacrolimus, everolimus, mycophenolate, gemfibrozil, insulin Isophane 40units BD, irbesartan, metoprolol, calcitriol, esomeprazole, magnesium supplements.
On examination, with a BMI of 23kg/m2 , she had ‘moon-like’ facies with minimal adipose tissue in her trunk and extremities consistent with familial partial lipodystrophy. Elevated jugular venous pressure (JVP) with peripheral oedema and bilateral lung crackles confirmed congestive cardiac failure.
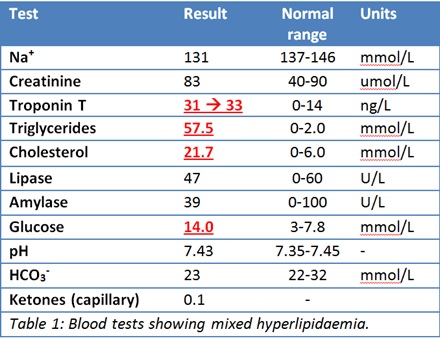
A visibly lipaemic serum sample showed very severe hypertriglyceridaemia, hypercholesterolaemia, mild hyperglycaemia and equivocal troponin. Lipase was normal.
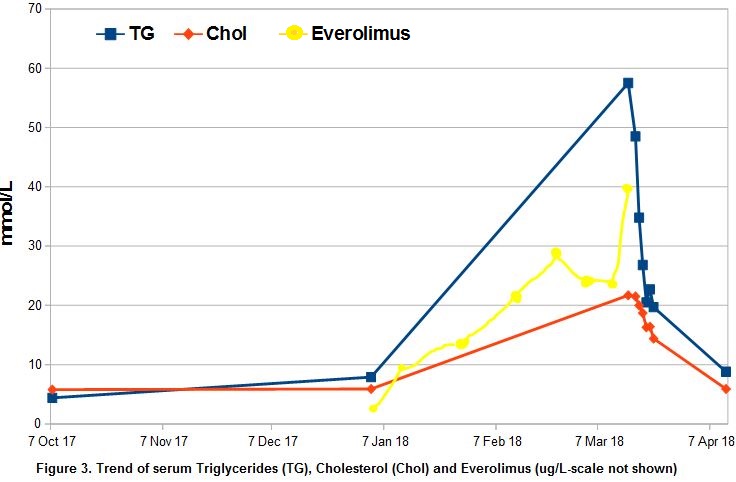
Current cholesterol and triglyceride level were out of proportion to usual levels. Prednisone dose was being reduced and Everolimus started over the past 5 months.
The patient was treated with insulin infusion, heparin infusion, fenofibrate, pravastatin, fish oil and withdrawal of everolimus.

Discussion:
Dunnigan type familial partial lipodystrophy is an autosomal dominant mutation of the LMNA gene leading to varying degrees of lipodystrophy and cardiomyopathy. Secondary causes of hypertriglyceridaemia should be considered if extent of hypertriglyceridaemia is above patient’s usual baseline.
Our patient had severe hypertrygliceridemia secondary to Everolimus similar to some previous reported cases. Treatment insulin infusion, fibrate therapy, statin, fish oil and nicotinic acid. Plasmapharesis has been used in some cases.
Learning Points:
- Severe hyperlipidaemia can present with congestive cardiac failure.
- Facial features of Dunningan type familial partial lipidystrophy can be Cushingoid.
- In familial hyperlipidaemia, further elevations of lipid levels suggest secondary causes.
- Prompt treatment of hypertriglyceridaemia is required to avoid pancreatitis.
- Lightbourne M, Brown RJ (2017) Genetics of Lipodystrophy. Endocrinol Metab Clin North Am. 2017 Jun;46(2):539-554. doi: 10.1016/j.ecl.2017.01.012.
- Berglund L, Brunzell JD, Goldberg AC, Goldberg IJ, Sacks F, et al. (2012); Evaluation and Treatment of Hypertriglyceridemia: An Endocrine Society Clinical Practice Guideline, The Journal of Clin Endocrin & Metab, Volume 97, Issue 9, 1 September 2012, Pages 2969–2989, https://doi.org/10.1210/jc.2011-3213
- Acharya GK, Hita AG, Yeung SJ, Yeung SJ. (2017) Diabetic Ketoacidosis and Acute Pancreatitis: Serious Adverse Effects of Everolimus. Ann Emerg Med. 2017 May; 69(5):666-667. doi: 10.1016/j.annemergmed.2017.01.002. Bär S, Daudel F, Zueger T (2017) Ominous triad triggered by high-dose glucocorticosteroid therapy. BMJ Case Rep. 2017 Jun 18; . pii: bcr-2017-220328. doi: 10.1136/bcr-2017-220328.
- Krawiec P, Mełges B, Pac-Kożuchowska E, Mroczkowska-Juchkiewicz A, & Czerska K (2016). Fitting the pieces of the puzzle together: a case report of the Dunnigan-type of familial partial lipodystrophy in the adolescent girl. BMC Pediatrics, 16, 38.